The PACT Act: Complete Veterans Guide
The Sergeant First Class Heath Robinson Honoring our Promise to Address Comprehensive Toxics Act of 2022 is the largest expansion of VA benefits in decades — covering burn pits, Agent Orange, radiation, and other toxic exposures for millions of veterans. This guide covers everything: who qualifies, every presumptive condition, how to file, and how to leverage a PACT Act service connection to build well-supported secondary claims — including sinusitis secondary to PACT Act allergic rhinitis.
What Is the PACT Act?
Signed into law on August 10, 2022, the PACT Act (P.L. 117-168) is the most significant expansion of VA disability benefits in a generation. Named after Army Specialist Heath Robinson, who died of a rare cancer linked to burn pit exposure in Iraq, the law addresses longstanding gaps in coverage for toxic exposures during military service — from burn pits in Afghanistan and Iraq to Agent Orange in Southeast Asia and radiation from nuclear testing.
Before the PACT Act, veterans had to individually prove that their cancers, respiratory diseases, and other conditions were caused by toxic exposure. The PACT Act removes that burden for covered conditions by establishing presumptive service connection — the law itself provides the nexus. If you served in a qualifying location and have a qualifying diagnosis, service connection must be granted. No nexus letter required for listed conditions.
The PACT Act does four major things:
- Creates presumptive service connection for burn pit and airborne hazard exposures for post-9/11 veterans who served in Southwest Asia and other qualifying locations
- Expands the locations where Agent Orange presumptive service connection applies, covering veterans in Thailand, Laos, Cambodia, Guam, Korea, and Johnston Atoll
- Adds new conditions to the Agent Orange presumptive list, including hypertension, hypothyroidism, and monoclonal gammopathy of undetermined significance (MGUS)
- Expands VA healthcare eligibility to cover most post-9/11 veterans regardless of discharge characterization
Official VA Source
This guide is an independent explainer. For the U.S. Department of Veterans Affairs' own overview of the law and your eligibility, see the official page: The PACT Act and your VA benefits (VA.gov).
Effective Date: File Now, Not Later
For most PACT Act claims, the earliest possible effective date is August 10, 2022 — the date the law was signed — unless you had a previously denied claim for the same condition. Filing an Intent to File (VA Form 21-0966) immediately locks in your effective date for up to one year while you gather evidence. Each month you wait is potentially a month of retroactive pay that starts later than it needs to.
Who Is Covered?
The PACT Act creates four distinct coverage groups. Understanding which group applies to you determines your available presumptive conditions and what evidence is needed.
Post-9/11 Veterans — Burn Pit & Airborne Hazards
Veterans who served on active duty on or after August 2, 1990 in Southwest Asia, Afghanistan, or other qualifying locations where airborne hazards or open burn pits were present. This is the largest group — covering millions of veterans from every era from Gulf War through Afghanistan.
Agent Orange — Newly Recognized Locations
Veterans who served at specific locations in Thailand, Laos, Cambodia, Guam, American Samoa, Johnston Atoll, or Korea during qualifying periods — previously unable to access Agent Orange presumptives — are now fully covered.
Agent Orange — New Conditions Added
Veterans already covered by Agent Orange presumptives (Vietnam, Korean DMZ, etc.) now have additional conditions added to the list: hypertension, hypothyroidism, MGUS, and Parkinson's-like tremor.
Radiation-Exposed Veterans
Veterans who participated in radiation-risk activities (nuclear weapons testing, Hiroshima/Nagasaki occupation, etc.) have new conditions added to the radiation exposure presumptive list, including ischemic heart disease and stroke.
Group 1: Burn Pit & Airborne Hazard Presumptives
Qualifying Service Locations
To qualify for burn pit and airborne hazard presumptives, you must have served on active duty (including active duty for training or inactive duty training) in one or more of the following locations during the applicable qualifying period. The qualifying date depends on where you served. Service in the airspace above any of these locations also qualifies. The VA has authority to add additional locations by regulatory determination.
On or after September 11, 2001
On or after August 2, 1990
PACT Act Cancer Presumptives — Head, Neck & Respiratory
If you served in a qualifying location and have been diagnosed with any of the following cancers, service connection is presumptive. You need only prove qualifying service and a current diagnosis. No nexus letter, no C&P examination to establish causation — the law provides the connection.
The table below pairs each cancer with the 38 CFR diagnostic code the VA uses to rate it once service connection is granted. As a rule, an active malignant tumor is rated 100% while it is active and for six months after treatment ends; the VA then schedules a mandatory re-examination and re-rates the condition on its residuals. Links open the governing rating schedule section on the official eCFR in a new tab.
| Presumptive Cancer | Diagnostic Code | How the VA Rates It |
|---|---|---|
| Cancer of the nasopharynx | DC 6819 · § 4.97 | Malignant neoplasm of the respiratory system: 100% while active and for 6 months after treatment ends, then rated on residuals. |
| Squamous cell carcinoma of the head or neck | DC 6819 · § 4.97 | Rated as a respiratory/upper-airway malignancy: 100% while active and for 6 months post-treatment, then on residuals. |
| Laryngeal cancer (voice box) | DC 6819 · § 4.97 | 100% while active and for 6 months after treatment, then on residuals (e.g., laryngectomy under DC 6518, voice loss under DC 6519). |
| Sinonasal cancer (sinuses and nasal cavity) | DC 6819 · § 4.97 | 100% while active and for 6 months after treatment ends, then rated on residuals. |
| Cancer of the trachea | DC 6819 · § 4.97 | 100% while active and for 6 months after treatment ends, then rated on residuals. |
| Cancer of the bronchus | DC 6819 · § 4.97 | 100% while active and for 6 months after treatment ends, then rated on residuals. |
| Lung cancer — all histologic types (adenocarcinoma, squamous cell, large cell, small cell) | DC 6819 · § 4.97 | 100% while active and for 6 months after treatment ends, then rated on residuals (loss of lung function under the General Rating Formula). |
| Malignant melanoma of the head, neck, or respiratory tract | DC 7833 · § 4.118 | 100% only if treatment is systemic (chemo, wide surgery, or X-ray beyond the skin); otherwise rated on scars/disfigurement under DC 7800–7805. |
PACT Act Cancer Presumptives — Other Solid Tumors
| Presumptive Cancer | Diagnostic Code | How the VA Rates It |
|---|---|---|
| Esophageal cancer | DC 7343 · § 4.114 | Malignant neoplasm of the digestive system: 100% while active and for 6 months after treatment ends, then on residuals. |
| Thyroid cancer (any type) | DC 7914 · § 4.119 | Malignant neoplasm of the endocrine system: 100% while active and for 6 months after treatment, then on residuals. |
| Kidney cancer / cancer of the renal pelvis | DC 7528 · § 4.115b | Genitourinary malignancy: 100%, with a mandatory exam 6 months after treatment, then rated on voiding or renal dysfunction, whichever predominates. |
| Cancer of the ureter | DC 7528 · § 4.115b | Genitourinary malignancy: 100%, then rated on voiding or renal dysfunction after the mandatory 6-month exam. |
| Bladder cancer / urothelial carcinoma | DC 7528 · § 4.115b | Genitourinary malignancy: 100%, then rated on voiding or renal dysfunction after the mandatory 6-month exam. |
| Gastrointestinal cancers (stomach, colon, rectal, small intestine, pancreatic, hepatic) | DC 7343 · § 4.114 | Malignant neoplasm of the digestive system: 100% while active and for 6 months after treatment, then on residuals. |
| Prostate cancer | DC 7528 · § 4.115b | Genitourinary malignancy: 100%, then rated on voiding or renal dysfunction after the mandatory 6-month exam. |
| Reproductive cancers (cervical, ovarian, uterine, testicular) | DC 7627 · § 4.116 / DC 7528 · § 4.115b | Gynecological cancers (cervical/ovarian/uterine) rate at 100% under § 4.116; testicular cancer rates at 100% under DC 7528. Both continue 6 months post-treatment, then on residuals. |
| Glioblastoma multiforme and other primary brain cancers | DC 8002 · § 4.124a | Malignant brain tumor: 100% continued for 2 years after treatment, then rated on neurological residuals with a 30% minimum. |
| Any other malignant melanoma | DC 7833 · § 4.118 | 100% only if treatment is systemic; otherwise rated on scars/disfigurement (DC 7800–7805) or impairment of function. |
| Any adenocarcinoma of the digestive system | DC 7343 · § 4.114 | Malignant neoplasm of the digestive system: 100% while active and for 6 months after treatment, then on residuals. |
PACT Act Cancer Presumptives — Blood & Hematologic Cancers
| Presumptive Cancer | Diagnostic Code | How the VA Rates It |
|---|---|---|
| Acute myeloid leukemia (AML) | DC 7703 · § 4.117 | 100% with active disease or during treatment; mandatory exam 6 months after treatment ends, then rated on residuals. |
| Chronic myeloid leukemia (CML) | DC 7719 · § 4.117 | Rated under its own code (carved out of DC 7703): 100% with active disease or during treatment, then on residuals. |
| Acute lymphoblastic leukemia (ALL) | DC 7703 · § 4.117 | 100% with active disease or during treatment, then re-examined and rated on residuals. |
| Chronic lymphocytic leukemia (CLL) | DC 7703 · § 4.117 | Symptomatic disease = 100%; asymptomatic CLL at Rai Stage 0 is rated 0%. Active disease/treatment is rated 100%, then on residuals. |
| Hairy cell leukemia and other B-cell neoplasms | DC 7703 · § 4.117 | Rated as leukemia: 100% with active disease or during treatment, then on residuals. |
| Non-Hodgkin's lymphoma (all subtypes) | DC 7715 · § 4.117 | 100% with active disease or during treatment; the mandatory re-exam comes 2 years after treatment ends, then rated on residuals. |
| Hodgkin's disease / Hodgkin's lymphoma | DC 7709 · § 4.117 | 100% with active disease or during treatment; mandatory exam 6 months after treatment, then rated on residuals. |
| Multiple myeloma | DC 7712 · § 4.117 | Symptomatic disease = 100%, continued 5 years from diagnosis; asymptomatic/smoldering disease is rated 0%. |
| Myelodysplastic syndromes (MDS) | DC 7725 · § 4.117 | 100% if requiring stem-cell transplant or chemotherapy; lower tiers (60%/30%) based on transfusion and infection frequency. |
| Waldenstrom's macroglobulinemia | DC 7715 · § 4.117 | No dedicated code; rated as an indolent non-Hodgkin's lymphoma — 100% with active disease or during treatment, then on residuals. |
| Any other hematologic malignancy the VA determines is associated with burn pit or toxic exposure | § 4.117 | Rated under the most closely analogous hemic/lymphatic code in § 4.117, generally 100% during active disease and treatment, then on residuals. |
PACT Act Presumptive Illnesses — Respiratory & Related
Beyond cancer, the PACT Act establishes presumptive service connection for a defined list of respiratory and related illnesses for burn pit and airborne hazard veterans. As with the cancer presumptives, you need only prove qualifying service and a current diagnosis — no nexus letter and no C&P opinion on causation is required. The following conditions are full PACT Act presumptives:
Unlike the cancers, these conditions are rated on severity — most under the General Rating Formulas of 38 CFR § 4.97, which key the percentage to pulmonary function testing (FEV-1, FEV-1/FVC, DLCO) and to how much treatment the condition requires. The diagnostic code and criteria for each are below.
| Presumptive Illness | Diagnostic Code | How the VA Rates It |
|---|---|---|
| Asthma that was diagnosed after service | DC 6602 · § 4.97 | 10/30/60/100% by FEV-1, FEV-1/FVC, attack frequency, and medication use (100% needs FEV-1 <40%, or daily systemic steroids/immunosuppressants). |
| Chronic bronchitis | DC 6600 · § 4.97 | 10/30/60/100% under the General Rating Formula for Restrictive/Obstructive disease (FEV-1, FEV-1/FVC, DLCO, exercise capacity, cor pulmonale). |
| Chronic obstructive pulmonary disease (COPD) | DC 6604 · § 4.97 | 10/30/60/100% on the same General Rating Formula thresholds as chronic bronchitis. |
| Chronic rhinitis | DC 6522 · § 4.97 | 30% with nasal polyps; 10% without polyps but with >50% obstruction of both passages or complete obstruction of one side. |
| Chronic sinusitis | DC 6510–6514 · § 4.97 | 0/10/30/50% under the General Rating Formula for Sinusitis, keyed to incapacitating episodes, antibiotic courses, and surgery. |
| Constrictive bronchiolitis or obliterative bronchiolitis | § 4.97 (by analogy) | No dedicated code; rated by analogy (most often the obstructive formula, DC 6600) on PFT severity. A surgical lung biopsy is often needed to confirm the diagnosis. |
| Emphysema | DC 6603 · § 4.97 | 10/30/60/100% on the same General Rating Formula thresholds as chronic bronchitis and COPD. |
| Granulomatous disease | § 4.97 (varies by type) | No single umbrella code; e.g., granulomatous rhinitis = DC 6524, pulmonary forms rated under the relevant lung-infection or restrictive formula. |
| Interstitial lung disease (ILD) | DC 6825 · § 4.97 | 10/30/60/100% under the Interstitial Lung Disease formula (FVC, DLCO, cor pulmonale, supplemental-oxygen requirement). |
| Pleuritis | DC 6845 · § 4.97 | Chronic pleural effusion or fibrosis, rated 10/30/60/100% under the Restrictive Lung Disease formula. |
| Pulmonary fibrosis | DC 6825 · § 4.97 | 10/30/60/100% under the Interstitial Lung Disease formula (FVC <50% or DLCO <40% or oxygen need = 100%). |
| Sarcoidosis | DC 6846 · § 4.97 | 0/30/60/100% by treatment intensity and organ involvement (100% for cor pulmonale or progressive disease despite treatment). |
Several of these conditions warrant a closer look — constrictive/obliterative bronchiolitis is one of the signature listed presumptives linked to burn pit inhalation, while constrictive pericarditis is a serious cardiac condition seen in exposed veterans that is not on the enumerated list and must be pursued with a nexus opinion:
Constrictive / Obliterative Bronchiolitis
A severe inflammatory lung disease causing scarring and permanent narrowing of the small airways (bronchioles). It is one of the signature conditions linked to burn pit inhalation. Unlike asthma, it does not respond to bronchodilators and can be irreversible. If you have unexplained fixed airflow obstruction post-deployment, pursue full pulmonary evaluation including surgical lung biopsy if necessary.
Constrictive Pericarditis
Chronic inflammation and fibrotic scarring of the pericardium (the fibrous sac surrounding the heart), restricting cardiac filling. Linked to toxic and particulate exposures, but not one of the enumerated PACT Act presumptive illnesses — it must be claimed through the broader airborne-hazard framework with a supporting nexus opinion. Symptoms include progressive dyspnea, lower extremity edema, and elevated venous pressure. Often requires pericardiectomy for definitive treatment.
Respiratory & Upper Airway Conditions — Presumptives and the Broader Airborne Hazard Framework
Several of the most commonly claimed respiratory and upper airway conditions — chronic rhinitis (including allergic rhinitis), chronic sinusitis, and post-service asthma — are now full PACT Act presumptives under the list above. For qualifying veterans that means the same low burden as the cancer presumptives: prove qualifying service and a current diagnosis. Beyond the enumerated conditions, the PACT Act also created a broader airborne hazard framework that supports service connection for related upper- and lower-airway conditions that are not specifically listed. The VA's own clinical guidance acknowledges that burn pit smoke, fine particulate matter (PM2.5), sand, dust, oil well fires, and chemical fumes during deployment cause a spectrum of upper and lower airway diseases.
Figure: Where inhaled airborne hazards settle in the respiratory tract. Larger particles and irritant gases are trapped high in the nose, sinuses and large airways, while the finest particulate matter (PM2.5 and smaller) is carried deep into the small airways and alveoli. Each depth of deposition maps to a cluster of PACT Act respiratory presumptives — from allergic rhinitis and sinusitis in the upper airway, to asthma, bronchitis and COPD in the bronchi, to constrictive bronchiolitis and interstitial lung disease deep in the lung. This is why a single exposure history can support claims for several distinct conditions.
Adapted from: Falvo MJ, Osinubi OY, Sotolongo AM, Helmer DA. "Airborne Hazards Exposure and Respiratory Health of Iraq and Afghanistan Veterans." Epidemiologic Reviews. 2015;37(1):116–130. doi:10.1093/epirev/mxu009 (PMID 25589052)
The conditions below are central to PACT Act respiratory claims — the first three are listed presumptives that also serve as strong foundations for secondary claims, while the final group covers related conditions pursued through the broader framework:
Chronic Rhinitis (incl. Allergic Rhinitis)
IgE-mediated and irritant-driven inflammation of the nasal mucosa triggered by airborne allergens and irritants encountered during deployment. Now a listed PACT Act presumptive and one of the most commonly granted conditions. Rated under DC 6522. Once service-connected, it is a strong foundation for secondary claims — most critically, sinusitis secondary to allergic rhinitis (see detailed case study below).
Chronic Sinusitis / Rhinosinusitis
Persistent inflammation of the paranasal sinuses, often developing as a direct consequence of chronic allergic rhinitis when sinus drainage is obstructed. Now a listed PACT Act presumptive; it can also be claimed as secondary to service-connected chronic/allergic rhinitis. Rated DC 6510-6514.
Asthma (Diagnosed After Service)
Reactive airway disease diagnosed after service with airborne hazard exposure is a listed PACT Act presumptive. Pre-existing mild asthma that worsened significantly during deployment may also qualify under aggravation theory. Rated DC 6602; often the gateway condition to secondary claims for sleep apnea and GERD.
Other Recognized Conditions
Laryngitis and chronic laryngeal irritation, laryngopharyngeal reflux (LPR), reactive airway dysfunction syndrome (RADS), exercise-induced bronchoconstriction, and vocal cord dysfunction are not on the enumerated presumptive list, but are documented sequelae of deployment-related airborne hazard exposure and can be pursued through the broader framework with a supporting nexus opinion.
Register with the Airborne Hazards and Open Burn Pit Registry
The VA maintains a free registry specifically for veterans exposed to airborne hazards and open burn pits. Completing the registry creates a contemporaneous record of your exposures and symptoms that significantly strengthens any future claims. It also triggers a VA health evaluation. Register through MyHealtheVet at VA.gov or call 1-800-827-1000 to be enrolled.
Group 2: Agent Orange — Newly Recognized Locations
Before the PACT Act, Agent Orange presumptive service connection applied primarily to veterans who served in Vietnam or in certain other limited locations. The PACT Act dramatically expanded geographic coverage. Veterans who served at the following locations and were previously denied Agent Orange claims can now file Supplemental Claims with these new locations as the legal basis:
| Location | Qualifying Service Period |
|---|---|
| Laos | December 1, 1965 – September 30, 1969 |
| Cambodia (Cambodian air bases) | April 16, 1969 – April 30, 1969 |
| Guam, American Samoa, or territorial waters | January 9, 1962 – July 31, 1980 |
| Johnston Atoll or vessels near Johnston Atoll | January 1, 1972 – September 30, 1977 |
| Republic of Korea — any U.S. or Korean military base | September 1, 1967 – August 31, 1971 |
| Thailand military bases (any RTAF base with significant U.S. presence) | January 9, 1962 – June 30, 1976 |
| Any location where Agent Orange was stored, tested, or used | Any period of service |
All traditional Agent Orange presumptive conditions apply to these newly recognized locations. If you served at any of these locations during the qualifying period and have a diagnosis of any Agent Orange presumptive condition (Parkinson's disease, peripheral neuropathy, ischemic heart disease, Type 2 diabetes, prostate cancer, Non-Hodgkin's lymphoma, multiple myeloma, AL amyloidosis, chloracne, porphyria cutanea tarda, and others), file or refile immediately.
Group 3: New Conditions Added to Agent Orange Presumptives
The PACT Act added several new conditions to the Agent Orange presumptive list. These are now presumptively service-connected for any veteran with qualifying Agent Orange exposure (Vietnam, Korean DMZ, or any of the newly expanded locations above):
As with the burn pit presumptives above, the table below pairs each newly added Agent Orange condition with the 38 CFR diagnostic code the VA uses to rate it once service connection is granted, and a short summary of how the rating works. Links open the governing rating schedule section on the official eCFR in a new tab. Deeper context for each condition follows beneath the table.
| New Agent Orange Presumptive | Diagnostic Code | How the VA Rates It |
|---|---|---|
| Hypertension (high blood pressure) | DC 7101 · § 4.104 | 10/20/40/60% by blood pressure: 10% for diastolic predominantly 100+, systolic 160+, or continuous medication with a history of diastolic 100+; 20% at diastolic 110+/systolic 200+; 40% at diastolic 120+; 60% at diastolic 130+. |
| Hypothyroidism (underactive thyroid) | DC 7903 · § 4.119 | Endocrine rating: 10% when continuous medication is required to control the condition, rising to 30/60/100% with documented symptoms (e.g., fatigue, weight gain, cognitive effects) and, at 100%, thyroid crisis or hospitalization. |
| Monoclonal gammopathy of undetermined significance (MGUS) | § 4.117 (by analogy) | No dedicated code; rated by analogy under the hemic and lymphatic schedule — generally 0% while asymptomatic and monitored. On progression to multiple myeloma it is rated under DC 7712 (100% with symptomatic disease, continued 5 years). |
| Parkinson's-like tremor (parkinsonism short of Parkinson's disease) | DC 8004 · § 4.124a | Parkinsonism carries a 30% minimum, with the individual disabling effects (tremor, rigidity, gait, speech) rated separately and combined. Full Parkinson's disease is the long-standing Agent Orange presumptive; this extends coverage to tremor short of that diagnosis. |
Hypertension
High blood pressure is now a presumptive for Agent Orange-exposed veterans — one of the most impactful additions. Millions of Vietnam veterans were denied hypertension claims for decades. Now it is presumptive. A hypertension diagnosis plus qualifying service equals service connection. Rated DC 7101; often the gateway to secondary claims for cardiac and renal conditions.
Hypothyroidism
Underactive thyroid function is now presumptive for Agent Orange-exposed veterans. Rated DC 7903 under § 4.119, beginning at 10% once continuous medication is required. Hypothyroidism opens the door to secondary claims for depression, fatigue, cognitive impairment, hyperlipidemia, and cardiac effects — all documented consequences of inadequately treated or subclinical hypothyroidism.
Monoclonal Gammopathy of Undetermined Significance (MGUS)
A precancerous blood condition characterized by abnormal protein in the blood that can progress to multiple myeloma. Rated by analogy under § 4.117 — generally 0% while asymptomatic and monitored. With MGUS service-connected, any subsequent progression to multiple myeloma (DC 7712) can be claimed as a direct continuation. Requires regular monitoring for progression.
Parkinson's-Like Tremor (Non-Parkinsonism)
Tremor and Parkinson's-like symptoms that do not meet full diagnostic criteria for Parkinson's disease are now covered. Rated as parkinsonism under DC 8004 (§ 4.124a) with a 30% minimum and the individual effects rated separately. Full Parkinson's disease was already an Agent Orange presumptive; the PACT Act extended coverage to the broader spectrum of parkinsonian features short of a definitive Parkinson's diagnosis.
How to File a PACT Act Claim
Step 1 — Determine Your Category and Confirm Qualifying Service
Before filing, identify which PACT Act group applies to you. Confirm qualifying service by reviewing your DD-214 for locations and dates. Deployment orders, unit records, and military occupational specialty records that place you in a qualifying location all strengthen your file. For burn pit exposure, document where you were stationed relative to burn pit operations. Complete the Airborne Hazards and Open Burn Pit Registry at VA.gov — this creates a formal record of your exposure claim.
Step 2 — Lock In Your Effective Date with an Intent to File
File an Intent to File (VA Form 21-0966) immediately if you are not ready to submit a complete claim. This preserves your effective date — the date from which back pay is calculated — for up to one year. You can file ITF online at VA.gov, by phone at 1-800-827-1000, or in person at a regional VA office. The ITF costs nothing and can be worth thousands of dollars in back pay if your claim takes months to develop.
Step 3 — Get Your Diagnosis Formally Documented
You must have a current diagnosis from a licensed medical professional. For cancer, this will be from an oncologist with pathology reports. For respiratory conditions, a pulmonologist, allergist, or ENT specialist. For Agent Orange conditions like hypertension, your primary care physician's documentation is sufficient. Ensure the diagnosis is recorded in VA treatment records, private medical records, or a completed Disability Benefits Questionnaire (DBQ). Do not rely on the VA's C&P examiner to diagnose your condition — have the diagnosis established before your exam.
Step 4 — File VA Form 21-526EZ
File your disability claim using VA Form 21-526EZ, "Application for Disability Compensation and Related Compensation Benefits." File online through VA.gov (which also automatically creates an ITF), through a free VSO (DAV, VFW, American Legion), by mail to your regional VA office, or in person. Clearly identify each condition as a PACT Act claim and note the qualifying location of service.
PACT Act Claim Evidence Checklist
- DD-214 showing service dates and qualifying deployment locations
- Deployment orders placing you in qualifying locations (if available)
- Current diagnosis documentation — VA records or private medical records
- Personal statement describing your exposure and the onset of symptoms (your account is competent lay evidence)
- Airborne Hazards and Open Burn Pit Registry enrollment confirmation
- Buddy statements from fellow veterans corroborating your exposure and service location
- Unit history or command chronologies documenting burn pit locations near your FOB or base
- For non-presumptive airborne hazard conditions: Private nexus letter connecting condition to deployment exposure
- For cancer claims: Pathology reports, oncology records, imaging reports
- For Agent Orange new location claims: Evidence of service in the specific qualifying location and time period
If You Were Previously Denied — Reopen With a Supplemental Claim
If you were denied a claim before August 10, 2022 for a condition that is now presumptive under the PACT Act, file a Supplemental Claim (VA Form 20-0995). The PACT Act itself — a change in law — constitutes new and relevant evidence that supports reopening a previously denied claim. In certain cases, the VA was required to automatically review previously denied PACT Act-eligible claims, but do not rely on the VA to act without your prompt. File your own Supplemental Claim to control your effective date.
For claims denied before August 10, 2022, there is a legal argument that the effective date should trace back to the date of the original denied claim — specifically under 38 USC § 5110(g), which addresses retroactive effective dates when service connection is established based on a liberalizing law. This is a nuanced legal question that a VSO or accredited VA claims agent can evaluate for your specific facts.
Secondary Service Connection: Building on Your PACT Act Connection
One of the most effective — and most underutilized — approaches in the VA system is secondary service connection. The PACT Act has made this approach available to millions of veterans who now have newly service-connected conditions that serve as the foundation for additional claims.
Under 38 CFR § 3.310, any condition that is caused or aggravated by a service-connected disability is itself service-connected — without needing to connect the secondary condition directly back to military service. The chain is: Military service → PACT Act presumptive service connection → Secondary condition caused by primary PACT Act condition → Secondary service connection.
Both the primary and secondary conditions receive separate disability ratings that combine under the whole-person formula, stacking on top of each other. A PACT Act primary condition that might rate at 10% can be the foundation for a 30% or higher secondary condition — significantly increasing total combined rating and monthly compensation.
The Secondary Service Connection Chain
Secondaries With the Most Medical Literature
The combinations below are the secondary connections that rest on the strongest published medical evidence — landmark clinical practice guidelines, large meta-analyses, and high-impact review articles. Each condition is paired with a primary, peer-reviewed source you (or your physician) can cite directly in a nexus letter. Connections that lacked solid published support have been deliberately left off this list, and each entry is labeled Strong (large meta-analytic or guideline-level support) or Moderate (consistent association, but the literature stops short of firm causation or notes a bidirectional relationship). Links open the source's full text or PubMed record in a new tab.
Allergic Rhinitis
Allergic rhinitis commonly precedes and predicts asthma — the "united airway" concept — with a roughly 3.8-fold increased risk of developing asthma.
Tohidinik HR, et al. World Allergy Organ J. 2019. Meta-analysis of 29 studies / 274,489 subjects — PMC full text. Framework guideline: ARIA 2016 revision (Brożek JL, J Allergy Clin Immunol) — PubMed.
Allergic rhinitis is a recognized predisposing and comorbid factor for chronic rhinosinusitis through ostiomeatal obstruction and shared mucosal inflammation; the definitive guideline treats the link as associative rather than firmly causal.
Fokkens WJ, et al. Rhinology 2020. European Position Paper on Rhinosinusitis (EPOS 2020) — PubMed.
Nasal obstruction from allergic rhinitis increases upper-airway resistance and is consistently associated with obstructive sleep apnea, with the strongest data in children.
Cao Y, et al. Medicine (Baltimore) 2018. Meta-analysis of allergic rhinitis and OSA — PMC full text.
Olfactory dysfunction is a recognized symptom of allergic rhinitis, reported in roughly 20–40% of patients and increasing with disease duration and severity.
Stuck BA, Hummel T. J Allergy Clin Immunol 2015. Systematic review of olfaction in allergic rhinitis — PubMed.
Asthma
Asthmatic airway inflammation, obesity, nasal obstruction, and steroid use promote upper-airway collapse during sleep; asthma patients develop OSA at roughly 2.6× the rate of non-asthmatics (DC 6847).
Kong DL, et al. Sci Rep 2017. Meta-analysis of 26 studies / 7,675 patients — PMC full text.
Refluxed acid reaches the airway by microaspiration or a vagally-mediated bronchoconstriction reflex; the association with asthma exacerbation is consistent but modest in magnitude.
Mallah N, et al. Pediatr Allergy Immunol 2022. Systematic review / meta-analysis (32 studies, >1.6M patients) — PubMed.
Living with episodic breathlessness and fear of attacks drives elevated anxiety; asthma patients carry roughly twice the odds of anxiety symptoms or disorders.
Ye G, et al. Psychol Med 2021. Meta-analysis of 19 studies / 106,813 participants — PubMed.
Asthma and depression clearly co-occur and interact bidirectionally to worsen control; nexus opinions should frame the relationship as a well-documented comorbidity rather than a one-directional cause.
Gao Y-H, et al. PLoS One 2015. Meta-analysis of depression and asthma — open-access full text.
Hypertension
Sustained high blood pressure accelerates atherosclerosis and raises myocardial oxygen demand, driving angina and myocardial infarction in a linear dose-response relationship.
Rapsomaniki E, et al. Lancet 2014. Lifetime cardiovascular risk in 1.25 million people — PMC full text.
Chronic pressure overload forces the left ventricle to thicken; this hypertensive target-organ change independently predicts cardiovascular events and mortality.
Zhang H, et al. J Clin Hypertens 2020. Meta-analysis of 9 studies / 41,870 hypertensive patients — PMC full text.
High arterial pressure damages the kidney's small vessels and glomeruli (nephrosclerosis), progressively reducing filtration.
Weldegiorgis M, Woodward M. BMC Nephrol 2020. Systematic review / meta-analysis (>2.3M people) — PMC full text.
Elevated blood pressure damages the retinal arterioles, producing the vascular narrowing, hemorrhages, and exudates that define the condition.
Wong TY, Mitchell P. N Engl J Med 2004. NEJM review on hypertensive retinopathy — PubMed.
Hypertension causes endothelial dysfunction and reduced penile blood flow; the association is strong and consistent, though partly entangled with antihypertensive medication effects.
Ning L, Yang L. Andrologia 2017. Meta-analysis of 40 studies / 121,641 subjects — PubMed.
Hypothyroidism
Low thyroid hormone reduces LDL-receptor clearance, raising total and LDL cholesterol; the effect is mechanistically established and reverses with levothyroxine.
Liu H, et al. Endocr Connect 2022. Review of dyslipidemia mechanisms in hypothyroidism — PMC full text.
Low thyroid hormone slows neurotransmitter activity and metabolism, contributing to depressed mood — a modest effect strongest in overt disease.
Bode H, et al. JAMA Psychiatry 2021. Meta-analysis of 25 studies / 348,014 participants — PubMed.
Myxedematous tissue deposition at the wrist can compress the median nerve; the association is real but modest and attenuates after adjusting for age, sex, and BMI.
Shiri R. Muscle Nerve 2014. Meta-analysis of 18 studies — PubMed.
Low thyroid hormone can impair nerve metabolism and myelin maintenance, producing a polyneuropathy independent of diabetes.
Luo Y, et al. Front Endocrinol 2026. UK Biobank cohort (498,417 participants) — full text.
Diabetes Mellitus Type 2
Chronic hyperglycemia damages peripheral nerves, producing the "stocking-glove" distal symmetric polyneuropathy; the ADA recommends screening every Type 2 patient at diagnosis. Bilateral involvement is separately ratable.
ADA Professional Practice Committee. Diabetes Care 2024. Standards of Care — Neuropathy & Foot Care — PMC full text.
Sustained high blood sugar damages the retina's small vessels; diabetic retinopathy is the leading cause of new blindness in adults aged 20–74.
Solomon SD, et al. Diabetes Care 2017. ADA Position Statement on diabetic retinopathy — PMC full text.
Diabetes damages the kidney's filtering units, causing protein leakage and declining function; CKD in a diabetic is attributed to diabetes unless another cause is evident.
KDIGO Diabetes Work Group. Kidney Int 2022. KDIGO Clinical Practice Guideline for diabetes in CKD — PubMed.
Diabetic vascular and nerve damage impairs the blood flow and signaling needed for erection; prevalence reaches ~66% in Type 2 diabetes.
Kouidrat Y, et al. Diabet Med 2017. Meta-analysis of 145 studies / 88,577 men — PubMed.
MGUS
MGUS is a premalignant plasma-cell condition that progresses to multiple myeloma or a related malignancy at roughly 1% per year — about 6.5× the rate of controls.
Kyle RA, et al. N Engl J Med 2018. 34-year Mayo Clinic cohort (1,384 patients) — PMC full text.
In IgM MGUS the monoclonal antibody can attack peripheral nerve myelin (often anti-MAG mediated); for IgG/IgA the link is weaker and causality must be individually established.
Chaudhry HM, et al. Mayo Clin Proc 2017. Review of monoclonal-gammopathy-associated neuropathy — PMC full text.
Some monoclonal proteins are directly nephrotoxic, damaging the kidney even when the plasma-cell clone is small — defined as monoclonal gammopathy of renal significance.
Leung N, et al. Nat Rev Nephrol 2019. International consensus report on MGRS — PMC full text.
Any Cancer
A cancer diagnosis and its treatment are a major psychological stressor; clinically significant depression, anxiety, or adjustment disorder occurs in a large minority of patients and survivors.
Mitchell AJ, et al. Lancet Oncol 2011. Meta-analysis of 94 interview-based studies — PubMed.
Neurotoxic agents (platinums, taxanes, vinca alkaloids) directly damage sensory nerves; neuropathy affects ~68% of patients early and ~30% beyond six months.
Seretny M, et al. Pain 2014. Systematic review / meta-analysis of 31 studies — PubMed.
Both the malignancy (chronic inflammation, marrow infiltration) and myelosuppressive chemotherapy/radiotherapy reduce red-cell production, with anemia prevalence reaching ~67% during treatment.
Ludwig H, et al. Eur J Cancer 2004. European Cancer Anaemia Survey (15,367 patients) — PubMed.
Cancer and its treatments produce persistent, disproportionate exhaustion via proinflammatory cytokines and HPA-axis/circadian disruption, often lasting into survivorship.
Berger AM, et al. J Natl Compr Canc Netw 2015. NCCN Cancer-Related Fatigue guideline — PMC full text.
Ischemic Heart Disease
Roughly 20% of patients hospitalized for an acute coronary syndrome meet criteria for major depression; the American Heart Association recognizes depression as a formal risk factor for poor cardiac prognosis.
Lichtman JH, et al. Circulation 2014. AHA Scientific Statement on depression after ACS — PubMed.
ED and coronary disease share the same endothelial atherosclerotic process; because penile arteries are smaller, ED typically precedes overt cardiac symptoms by 2–3 years.
Vlachopoulos C, et al. Circ Cardiovasc Qual Outcomes 2013. Meta-analysis of cohort studies — PubMed.
Ischemic damage and atrial remodeling create the electrical substrate that triggers and sustains atrial fibrillation; the relationship is well described but bidirectional.
Liang F, et al. Am J Physiol Heart Circ Physiol 2021. Review of coronary disease and atrial fibrillation — PubMed.
Intermittent nocturnal hypoxia and sympathetic surges accelerate coronary atherosclerosis; the association shows a severity-dependent gradient, though it is partly confounded by shared risk factors.
Craciun M-L, et al. Medicina (Kaunas) 2025. Meta-analysis of 18 prospective cohorts — PMC full text.
A note on this evidence: A Moderate rating does not mean a claim will fail — it means the published literature establishes a consistent association while stopping short of proven one-directional causation, often because the relationship runs both ways. These connections are still well worth pursuing; they simply call for a nexus letter that frames the link as a documented medical relationship and explains the mechanism in the individual veteran's case rather than asserting certainty.
Secondary Claims Require No New Service Evidence
When filing a secondary claim, you never need to go back and prove anything additional about your military service. The service connection for the primary PACT Act condition does all the heavy lifting. You need only: (1) a current diagnosis of the secondary condition from a licensed provider, and (2) a medical nexus opinion connecting the secondary condition to the primary service-connected condition. The service link is already established.
Case Study: Sinusitis Secondary to PACT Act Allergic Rhinitis
The following case study documents how a veteran successfully established secondary service connection for chronic sinusitis based on a PACT Act service-connected allergic rhinitis — the exact claim pathway the creator of this site followed. It illustrates the complete strategy, the evidence required at each step, and the medical framework that makes this connection well-established.
Chronic Sinusitis Secondary to Service-Connected Allergic Rhinitis (PACT Act)
Background: Veteran served in Southwest Asia with significant burn pit and airborne hazard exposure during multiple deployments. During and following deployment, the veteran developed persistent nasal congestion, postnasal drip, sneezing, and nasal itching — classic allergic rhinitis. Following return from service, recurring facial pressure, headaches, and mucopurulent nasal discharge began, with multiple courses of antibiotics required each year. Formal diagnoses: allergic rhinitis and chronic sinusitis.
Step 1 — Establishing PACT Act Direct Service Connection (Allergic Rhinitis): The veteran filed for allergic rhinitis as a direct service connection under the PACT Act airborne hazard framework, citing qualifying deployment to Afghanistan. Evidence included: DD-214 confirming service in Afghanistan post-2001, enrollment in the Airborne Hazards and Open Burn Pit Registry, a personal statement describing proximity to burn pit operations and the onset of nasal symptoms during deployment, and a private nexus letter from a board-certified allergist stating: "It is at least as likely as not that the veteran's allergic rhinitis was caused by sustained exposure to airborne particulate matter, combustion byproducts, and chemical irritants during deployment to Southwest Asia." VA granted service connection for allergic rhinitis, rated 10% under Diagnostic Code 6522.
Step 2 — Secondary Claim for Chronic Sinusitis (38 CFR § 3.310): With allergic rhinitis now service-connected, the veteran filed a secondary claim for chronic sinusitis. Evidence submitted: current VA medical records showing recurrent sinusitis diagnoses, CT scan of paranasal sinuses showing mucosal thickening and bilateral maxillary/ethmoid opacification, documentation of multiple prolonged courses of antibiotic treatment (each lasting four to six weeks) in the preceding year, along with records of headaches, facial pain, and purulent discharge associated with non-incapacitating sinusitis episodes, and a private nexus letter from the treating ENT surgeon stating that chronic sinusitis was "at least as likely as not" caused by the service-connected allergic rhinitis, with a detailed explanation of the ostiomeatal complex obstruction mechanism.
Result: VA granted secondary service connection for chronic pansinusitis under Diagnostic Code 6510-6522 (chronic pansinusitis, secondary to service-connected allergic rhinitis). Rating assigned at 30% under the General Rating Formula for Sinusitis (38 CFR § 4.97), which requires either: three or more incapacitating episodes per year of sinusitis requiring prolonged (lasting four to six weeks) antibiotic treatment, or more than six non-incapacitating episodes per year of sinusitis characterized by headaches, pain, and purulent discharge or crusting. Combined with the primary 10% allergic rhinitis rating under DC 6522, the veteran's combined rating increased materially.
The combination of (1) an existing PACT Act direct service connection for allergic rhinitis, (2) documented sinusitis with CT imaging and treatment records, and (3) a private nexus letter from a treating specialist explaining the specific medical mechanism made this claim straightforward to grant. This made the claim much harder to dismiss as speculative when a treating ENT provided a well-reasoned opinion citing the established medical relationship between allergic rhinitis and chronic sinusitis.
Why Sinusitis Secondary to Allergic Rhinitis Works: The Medical Mechanism
The medical connection between allergic rhinitis and chronic sinusitis is one of the most thoroughly documented causal relationships in upper airway medicine. Understanding this mechanism helps you and your physician write a nexus letter that is well-supported and difficult for the VA to set aside:
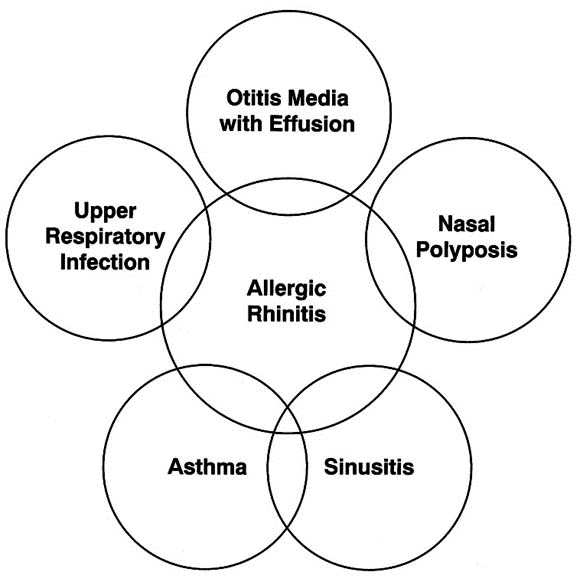
Figure: Comorbid conditions associated with allergic rhinitis. The overlapping circles illustrate the clinically documented relationships between allergic rhinitis and sinusitis, asthma, nasal polyposis, otitis media with effusion, and upper respiratory infections — each of which may qualify as a secondary service-connected condition under 38 CFR § 3.310.
Adapted from: Spector SL. "Overview of comorbid associations of allergic rhinitis." Journal of Allergy and Clinical Immunology. 1997;99(2):S773–S780. doi:10.1016/S0091-6749(97)70126-X
Ostiomeatal Complex Obstruction
Allergic rhinitis produces mucosal edema (swelling) and hypersecretion that physically obstructs the ostiomeatal complex — the narrow drainage pathways through which the paranasal sinuses ventilate and drain. Obstruction creates an anaerobic, stagnant environment in the sinus cavities that is directly conducive to bacterial colonization and infection.
Impaired Mucociliary Clearance
Allergic inflammation damages the cilia that sweep debris and pathogens out of the upper airways. With impaired mucociliary clearance, bacteria and allergens that would normally be cleared instead accumulate in the sinuses, driving chronic infection and inflammation.
Continuous Mucosal Inflammation
The same Th2 immune response driving allergic rhinitis extends continuously into the sinus mucosa — sinus epithelium is a direct anatomical extension of nasal mucosa. Allergic inflammation in the nose equals allergic inflammation in the sinuses, regardless of secondary infection.
Supported by Medical Literature
Multiple peer-reviewed studies document 40–80% co-prevalence of allergic rhinitis and sinusitis. Spector (1997) documented the comorbid associations of allergic rhinitis — including sinusitis, asthma, nasal polyposis, and otitis media — as clinically established conditions sharing common pathogenic mechanisms. The European Position Paper on Rhinosinusitis (EPOS 2020) and the American Academy of Otolaryngology guidelines both recognize allergic rhinitis as a major risk factor for chronic rhinosinusitis. This connection is well-supported enough that a properly reasoned specialist opinion should carry meaningful evidentiary weight.
Building Your Secondary Claim Nexus Letter
The nexus letter is the linchpin of every secondary claim. For a PACT Act secondary claim, it connects the secondary condition to the primary service-connected PACT Act condition. The VA rater's job is to weigh this letter against any C&P examiner opinion. A well-constructed private nexus letter from a relevant specialist routinely outweighs a cursory C&P examiner opinion.
A Strong Secondary Nexus Letter Includes:
- The exact legal phrase: "at least as likely as not" caused or aggravated by
- The name of the primary service-connected condition (with its diagnostic code/rating if known)
- The name and current diagnosis of the secondary condition
- The specific medical mechanism — HOW the primary condition causes or aggravates the secondary
- Citation of supporting peer-reviewed medical literature
- Confirmation that the physician reviewed the veteran's VA and/or private medical records
- The physician's credentials, board certifications, and relevant specialty
- Ideally, written by the veteran's treating specialist (treating provider opinions carry more weight)
A Weak Nexus Letter Will Fail:
- "Possibly related," "may be related," or "could be associated" — legally insufficient language
- Conclusion stated without explaining the medical mechanism or rationale
- Written by a physician in an unrelated specialty
- Does not reference the primary service-connected condition
- Not based on a review of the veteran's actual medical records
- "Reasonable degree of medical certainty" language without specifying 50%+ probability
- Fails to address the specific diagnostic question the VA requires
Model Nexus Language — Sinusitis Secondary to Allergic Rhinitis
Have your treating ENT, allergist, or pulmonologist adapt this language to your specific medical history. The mechanism section should reflect your actual clinical findings:
"It is my medical opinion that it is at least as likely as not (50% or greater probability) that [Veteran's Name]'s current diagnosis of chronic [maxillary / ethmoid / pansinusitis — specify] is caused by and/or aggravated by his/her service-connected allergic rhinitis [rated at __% under Diagnostic Code 6522].
Allergic rhinitis produces mucosal edema and increased mucous production that obstructs the ostiomeatal complex — the narrow drainage channels through which the paranasal sinuses ventilate and drain. This obstruction impairs sinus ventilation, creating the anaerobic conditions that facilitate bacterial colonization and recurrent sinusitis. Allergic inflammation also directly extends into the sinus epithelium through anatomical continuity of the upper airway mucosa, producing independent inflammatory disease in the sinuses separate from any infectious process.
These mechanisms are well-established in the medical literature. The European Position Paper on Rhinosinusitis and Nasal Polyps 2020 (EPOS 2020) and prospective cohort studies consistently demonstrate co-prevalence of allergic rhinitis and chronic rhinosinusitis exceeding 40-80%. Allergic rhinitis is recognized as a primary risk factor for the development and persistence of chronic sinusitis in peer-reviewed otolaryngology and allergy/immunology literature.
This opinion is based on my direct examination and ongoing treatment of [Veteran's Name], review of his/her medical records including VA treatment records, sinus CT imaging dated [date], and prior treatment documentation, and my [X] years of training and experience as a board-certified [Otolaryngologist / Allergist-Immunologist / ENT Surgeon]."
Sinusitis Rating: How the VA Rates Your Condition
Once service connection is established for chronic sinusitis — whether directly or as a secondary condition — the VA rates it under the diagnostic codes below. Understanding these criteria before your C&P exam helps you document your symptoms accurately and completely.
| Rating | Criteria — Pansinusitis (DC 6510) or Individual Sinus Groups |
|---|---|
| 50% | Following radical surgery with chronic osteomyelitis, or; near constant sinusitis characterized by headaches, pain and tenderness of affected sinus, and purulent discharge or crusting after repeated surgeries |
| 30% | Three or more incapacitating episodes per year of sinusitis requiring prolonged (lasting four to six weeks) antibiotic treatment, or; more than six non-incapacitating episodes per year of sinusitis characterized by headaches, pain, and purulent discharge or crusting |
| 10% | One or two incapacitating episodes per year of sinusitis requiring prolonged (lasting four to six weeks) antibiotic treatment, or; three to six non-incapacitating episodes per year of sinusitis characterized by headaches, pain, and purulent discharge or crusting |
| 0% | Detected by X-ray only |
"Incapacitating Episode" — the CFR Definition
Per 38 CFR § 4.97, an incapacitating episode of sinusitis means one that requires bed rest and treatment by a physician. Keep a symptom diary documenting every course of antibiotics (especially prolonged courses lasting four to six weeks), every episode requiring bed rest, and every episode characterized by headaches, pain, and purulent discharge or crusting. Your VA treating providers and private physicians should document these episodes in clinical notes — this documentation directly determines whether you are rated at 10%, 30%, or 50%.
Multiple Sinus Groups — Stack Your Ratings
The VA rates each affected sinus group separately under different diagnostic codes: maxillary sinuses (DC 6511), frontal sinuses (DC 6512), ethmoid sinuses (DC 6513), sphenoid sinuses (DC 6514), or pansinusitis involving multiple groups (DC 6510). If imaging shows involvement of multiple sinus groups, you may be entitled to separate ratings for each that then combine under the whole-person formula. Ensure that any sinus CT scan documents which specific sinus groups show mucosal thickening, air-fluid levels, or opacification.
C&P Exam Guidance for PACT Act Claims
For Listed Presumptive Conditions (Cancers and Respiratory Illnesses)
If your condition is one of the enumerated PACT Act presumptives — a listed cancer or one of the listed respiratory illnesses (asthma diagnosed after service, COPD, chronic bronchitis, chronic rhinitis, chronic sinusitis, emphysema, sarcoidosis, and the others) — the C&P examiner should only need to confirm: (1) your qualifying service in a PACT Act location, and (2) your current diagnosis. The examiner should not be asking for a nexus opinion — the law already provides the nexus. If the examiner's report opines that the condition is "less likely than not" related to service, that is a legal error under the PACT Act. Note it in your decision review request and challenge the adequacy of the examination under the standard established in Barr v. Nicholson, 21 Vet. App. 303 (2007).
For Non-Listed Airborne Hazard Conditions
For respiratory or upper-airway conditions claimed through the broader airborne hazard framework rather than as listed presumptives (for example LPR, RADS, or vocal cord dysfunction), the C&P examiner will evaluate nexus. Prepare to support the examiner's evaluation:
- Bring documentation of deployment to qualifying locations (orders, DD-214)
- Describe burn pit and airborne hazard exposures in specific detail — location, proximity, frequency, duration, the smell of smoke, eye and throat irritation that occurred during exposure
- Describe exactly when symptoms first appeared — ideally during or within months of deployment
- Describe the full progression of symptoms from first onset to current status
- Be thorough and accurate about your symptoms. Describe your day-to-day limitations, including flare-ups and more difficult periods — not just your better days
- Mention every medication you take, every specialist visit, every emergency room visit related to the condition
- If you already submitted a private nexus letter, confirm with your VSO that it is in your claims file before the exam date
For Secondary Claims at C&P Exam
When a secondary claim goes to C&P, the examiner evaluates: (1) whether the secondary condition currently exists, and (2) whether there is a medical connection between the secondary condition and the primary service-connected condition. Your primary job at this exam is to ensure the examiner has your complete file including the private nexus letter, and to document functional impact thoroughly.
- Clearly state which service-connected condition is the claimed cause of the secondary condition
- Describe how the secondary condition affects your daily functioning — describe inability to work, sleep disruption, missed activities, social limitations
- For sinusitis specifically: mention every antibiotic course in the past 12 months, every incapacitating episode, all CT imaging you have had, whether polyps have been identified, and any surgical procedures (FESS, etc.) that have been discussed or performed
- Confirm that the examiner reviews your private nexus letter during the examination
- Request a copy of the DBQ the examiner completes — this is your file and you are entitled to it
Common PACT Act Denials and How to Respond
Denial: "Veteran Did Not Serve in a Qualifying Location"
Request your complete service personnel file and all deployment records. Unit history records, command chronologies, AAFES records with overseas purchase tax exemptions, and military email records all document deployment locations. Buddy statements from fellow service members who served alongside you can corroborate qualifying service. A VSO can assist in requesting records through official VA channels. If records were lost in the 1973 NPRC fire or a subsequent records loss event, the VA must accept lay testimony under Buchanan v. Nicholson.
Denial: "Condition Not Among Listed Presumptives"
For cancer claims: verify that your specific histologic cancer type is covered under the PACT Act list. Some cancers not explicitly listed may still be covered — the VA Secretary has authority to recognize additional conditions. If your exact cancer type is not listed, pursue service connection through direct nexus with a private medical opinion connecting the cancer to toxic exposure. For respiratory illnesses: confirm whether your diagnosis is on the listed presumptive illnesses (asthma diagnosed after service, chronic bronchitis, COPD, chronic rhinitis, chronic sinusitis, constrictive/obliterative bronchiolitis, emphysema, granulomatous disease, interstitial lung disease, pleuritis, pulmonary fibrosis, or sarcoidosis) — if it is, and you have qualifying service, the denial is reversible on its face and should be challenged directly. For conditions not on any presumptive list, you can still establish service connection through the airborne hazard direct service connection pathway with a strong private nexus letter.
Denial: "No Nexus Between Secondary Condition and Primary Condition"
This is the most common — and most fixable — secondary claim denial. The VA's C&P examiner issued an opinion that the secondary condition is "less likely than not" caused by the primary PACT Act condition, or that "a nexus cannot be established without resort to speculation." Counter this with a private nexus letter from a treating specialist in the relevant field that: (1) reaches the "at least as likely as not" threshold, (2) explains the specific medical mechanism in detail, and (3) cites supporting medical literature. File a Supplemental Claim (VA Form 20-0995) with the private nexus letter as new and relevant evidence. The VA is not expected to simply prefer an inadequate C&P opinion over a well-reasoned private specialist opinion without explaining why — if the opinions are in equipoise, the benefit of the doubt goes to the veteran under 38 CFR § 3.102.
Denial: "Claim Was Denied Without a C&P Examination"
Under McLendon v. Nicholson, 20 Vet. App. 79 (2006), the VA is required to provide a C&P examination whenever there is competent evidence of a current disability, an in-service event or service-connected primary condition, and some indication of a possible nexus. If the VA denied your PACT Act claim without scheduling an exam at all, this is a failure of the VA's duty to assist under 38 CFR § 3.159. Challenge this in a Higher-Level Review, noting that the VA failed to provide an adequate examination as required by McLendon and the duty to assist statute.
Denial: "C&P Exam Was Inadequate"
A C&P exam is inadequate if the examiner: did not review the complete claims file, failed to address a specific Caluza Triangle element, provided only a conclusion without rationale, relied on an inaccurate history, or was performed by a contractor without relevant specialty. An inadequate exam is not considered sufficient evidence against the veteran. Challenge the exam's adequacy in a Higher-Level Review under Barr v. Nicholson, 21 Vet. App. 303 (2007), which requires that a C&P examination be based on a review of the claims file and provide a complete rationale.
Appeal Within One Year — Every Time
You have exactly one year from the date on your rating decision to appeal without losing your effective date. Missing this deadline forces a new claim with a new effective date, potentially losing years of back pay. After receiving any denial, immediately evaluate your appeal options: Supplemental Claim (best when you have new evidence), Higher-Level Review (best when the rater made a factual or legal error on the existing record), or BVA appeal (best for complex legal arguments). A VSO can help you choose the right lane — this service is always free.
PACT Act Healthcare Benefits
The PACT Act also dramatically expanded VA healthcare eligibility for veterans who were previously excluded due to income thresholds, insufficient service-connected conditions, or discharge characterization issues. Healthcare enrollment is separate from disability compensation — you should pursue both.
- Post-9/11 veterans with toxic exposure: Veterans who served on active duty after August 2, 1990 and have a qualifying toxic exposure are eligible for VA healthcare enrollment during a 10-year window after discharge, regardless of income. Discharge other than honorable does not automatically disqualify you (absent dishonorable discharge)
- Free care for toxic-exposure related conditions: Veterans enrolled under PACT Act provisions who do not yet have a service-connected rating receive VA care at no cost for conditions related to their toxic exposure
- Combat-related veteran healthcare: Veterans with combat service on or after November 11, 1998 have five years of free VA healthcare following discharge, now extended under PACT Act provisions
Enrolling in VA healthcare builds a treatment record. VA clinical documentation of your conditions — especially when it predates or coincides with your disability claims — is strong evidence. Get enrolled, get seen, and get your conditions formally documented in VA medical records before or alongside filing disability claims.
Key Regulations to Cite in Your Claims
Citing the specific federal statutes and regulations governing your PACT Act claim signals to raters that you understand the legal framework — and makes it harder for the VA to misapply the law:
- 38 USC § 1120 — The primary PACT Act statutory provision creating burn pit/airborne hazard presumptive service connection
- 38 CFR § 3.320 — Claims based on exposure to toxic substances, chemicals, and airborne hazards; the primary regulation implementing PACT Act burn pit and airborne hazard presumptive service connection
- 38 CFR § 3.317 — Compensation for certain disabilities occurring in Persian Gulf veterans; covers undiagnosed illnesses, medically unexplained chronic multi-symptom illnesses (Gulf War illness), and qualifying chronic disabilities
- 38 CFR § 3.310 — Secondary service connection; governs all secondary claims including sinusitis secondary to rhinitis
- 38 CFR § 3.102 — Benefit of the doubt; when evidence is in approximate equipoise, it shall be decided in the veteran's favor
- 38 CFR § 3.303 — Direct service incurrence; relevant for non-presumptive airborne hazard conditions
- 38 CFR § 4.97 — Rating schedule for respiratory conditions; Diagnostic Codes 6510-6522 govern sinusitis and rhinitis ratings
- 38 CFR § 3.159 — VA's duty to assist; requires the VA to obtain records and provide examinations before denying claims
PACT Act Secondary Claim (Sinusitis) Master Checklist
- PACT Act direct claim filed and service connection granted for primary condition (e.g., allergic rhinitis)
- Rating decision for primary condition received and reviewed for diagnostic code and percentage
- Formal diagnosis of secondary condition documented in medical records (VA or private)
- CT scan of paranasal sinuses obtained — documents affected sinus groups and mucosal changes
- Antibiotic treatment records for all sinusitis episodes in past 12 months compiled
- Symptom journal maintained documenting incapacitating episodes and non-incapacitating episodes with discharge
- Private nexus letter obtained from treating ENT or allergist reaching "at least as likely as not" standard
- Nexus letter includes specific medical mechanism (ostiomeatal complex obstruction, impaired cilia) and cites medical literature
- Intent to File (VA Form 21-0966) submitted to lock in effective date
- VA Form 21-526EZ filed with secondary claim language citing 38 CFR § 3.310
- All evidence uploaded to VA.gov eFile or provided to VSO before C&P exam
- C&P exam completed — described symptoms accurately including flare-ups, all antibiotic courses, all incapacitating episodes
Related Resources on This Site
Build on this guide with: Building a Strong Claim for comprehensive evidence strategy and nexus letter guidance. The Caluza Triangle to understand service connection at its foundation. The C&P Exam Guide for full preparation guidance. The Appeals Guide if your PACT Act or secondary claim is denied. And CFR & M21-1 Regulations for the full regulatory framework behind these claims.